


“Reputation management” used to be a term and responsibility that fell solely within the province of public relations. Yet with the changing healthcare landscape influencing how various stakeholders interact with healthcare organizations, today the term implies far more than it once did. Reputation management needs a more expansive description of what it entails — and a closer look at a tool that can be used in its service to ultimately attract patients, physicians, and potential partnering organizations.
The reputation ecosystem
Reputation building is nothing new for healthcare providers, as most have been trumpeting awards, quality outcomes, and accreditations for years to do this. What is more recent, however, is the growing complexity of what Movéo calls the “reputation ecosystem,” including new players and layers that can often mitigate — if not blunt — the direct efforts providers used to count on to build reputation.
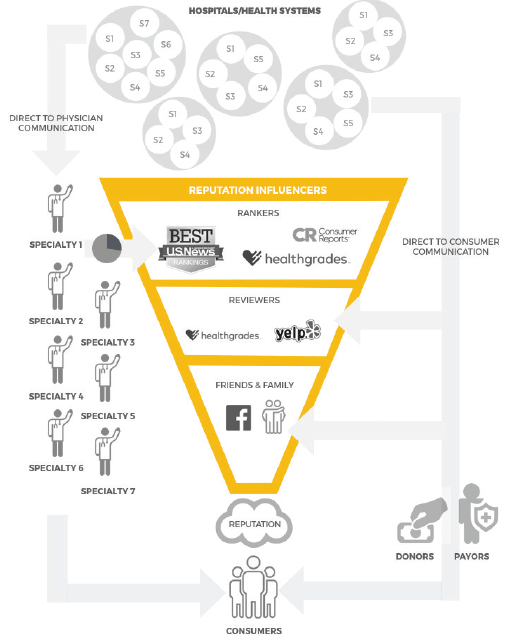 While direct to consumer communication remains a viable tool, it is no longer the onesided conversation it once was. Powerful reputation influencers abound, including ranking “authorities” (such as U.S. News & World Report, Consumer Reports, Leapfrog, and Healthgrades) and various review sites (foremost among them being Yelp). These sources of information combine with the pre-existing opinions and anecdotal experiences of friends and family members (now also amplified with social media “megaphones” like Facebook or Twitter) to influence decision.
While direct to consumer communication remains a viable tool, it is no longer the onesided conversation it once was. Powerful reputation influencers abound, including ranking “authorities” (such as U.S. News & World Report, Consumer Reports, Leapfrog, and Healthgrades) and various review sites (foremost among them being Yelp). These sources of information combine with the pre-existing opinions and anecdotal experiences of friends and family members (now also amplified with social media “megaphones” like Facebook or Twitter) to influence decision.
The net result is not as much a filtration of hospital and health system communication, but an entirely new stream of credible and (mostly) independent third-party information that is added to it.
Hospital reputation, then, is increasingly an amalgamation of these two independent
communication flows combined with whatever opinions might be shared by treating physicians. It falls on the healthcare consumer to deconflict these sources if necessary.
Direct to physician communication
If this ecosystem is not complex enough already, there is another significant element with which healthcare reputation managers need to contend — direct to physician communication.
Again, hospitals and health systems communicating with physicians is nothing new. However, in the past, it has been primarily done for three reasons:
- To help physicians on staff or affiliated with the hospital understand and believe in organizational strategy, drive change, or boost workplace satisfaction.
- For recruitment (i.e., to reduce the time to hire as well as bring more qualified potential physician candidates to the table).
- To strengthen relationships between physicians and a hospital or health system with the goal of driving more referrals in-network.
Today, however, there is another reason to communicate directly with physicians. And not just locally, but to the over 800,000 board-certified physicians practicing across the country — reputation management.
“What’s up, doc? Our ranking!”

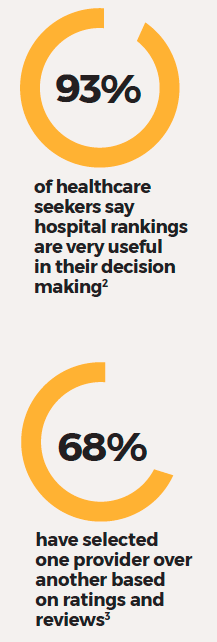
Each summer, U.S. News & World Report releases its influential list of the best hospitals in the nation. Like or hate them, consumers find these hospital rankings useful in that they give patients information about the institutions they trust with their lives. As a result, a lot of money and time are invested by providers participating in the ranking surveys — to say nothing of the advertising “arms race” that occurs post-publication.
But that advertising is typically created for and directed to consumers and not physicians (although it may also be collaterally received by them and other important audiences such as payors, donors, and partners).
This is significant, because U.S. News’ annual rankings are determined by an index of quality based on objective and subjective measures. We italicize subjective because a recent study1 confirmed that reputation has a more significant influence on the total U.S. News score than its objective counterparts.
 According to U.S. News, just shy of 30 percent of their score calculation comes from “expert opinion” — board-certified physicians across the country in the 16 specialities ranked in the the Best Hospitals issue are invited to list up to five hospitals they consider to be the best in their area of expertise for complex or difficult cases. The figures displayed in the rankings represent the average percentages of responding specialists over the last three years who named hospitals.
According to U.S. News, just shy of 30 percent of their score calculation comes from “expert opinion” — board-certified physicians across the country in the 16 specialities ranked in the the Best Hospitals issue are invited to list up to five hospitals they consider to be the best in their area of expertise for complex or difficult cases. The figures displayed in the rankings represent the average percentages of responding specialists over the last three years who named hospitals.
Due to this methodology, physicians have an outsized role in determining hospital reputations. This had led many hospitals to now target them in communication programs designed to increase awareness of and preference for their institution, service lines and “rock star” physicians. One academic hospital we recently encountered had $3MM+ dedicated to this task alone.
Looking back to the reputation ecosystem, you can see why we’ve added a “direct to physician” arrow, by specialty, coming from providers. The rub is, however, communicating with physicians is decidedly different than communicating with consumers. In general, physicians are better informed, more skeptical, and are typically more opinionated than the latter. In fact, they can tune out “consumer-centric” messaging in a flash and be lastingly put off by perceived “marketing fluff.” In the specialty realm, they are often more interested in what a specific peer is doing than the hospital where the peer is doing it. In fact, they may not be able to even name it.
For most hospitals and healthcare systems, reaching and influencing specialty physicians does not fall under the purview of “business as usual.”
Enter the physician specialty persona
A persona is a qualitative tool used to create a composite character that acts as an archetype to guide communication. Often based on multiple inputs, a persona brings the abstract concept of a targeted audience to life.
Personas typically include demographic, technographic, psychographic, and geographic information as well as personal narrative elements that create a comprehensive picture of a group’s behaviors, environment, motivations, and needs.
Sophisticated health systems have used consumer personas for things like website development or media targeting for years, but physician specialty personas are something new for most. At Movéo, we believe they can be a useful tool in hospital reputation management. In context, they are particularly helpful in the process of defining the underlying points of differentiation between physician specialties for the purpose of developing tailored reputation communications.
By using personas, we are able to humanize data to develop messages that appeal to specific audiences. What’s more, they allow us to avoid utilizing internal stakeholders as physician specialty proxies — a practice that often results in stereotyping (“our Dr. Jones is a ‘type A’ personality so his colleagues across the country must be too”).
“Head cases”
Let’s say a hospital wishes to enhance its reputation for neurology/neurosurgery. Constructing a persona can yield important insights about this specialty that can enable it to do so. Here’s how to go about it: Geo-, demo-, and technographic dimensions
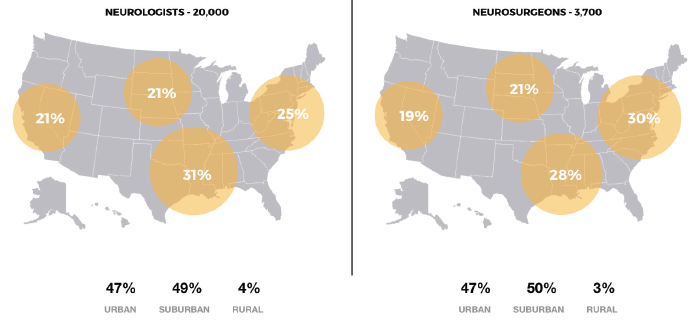
Geographically, neurologists/ neurosurgeons mirror each other very closely in where they practice across the country (sightly more in the South and East than the West and Midwest/47 percent located in urban areas for both). The major difference is their respective numbers. There are about 20,000 neurologists nationally, but only about one-fifth as many neurosurgeons.
Demographically, they align quite closely in age breakdowns and both specialties skew heavily male. Neurosurgery, however, is almost exclusively male (91 percent).
Neurologists and neurosurgeons are so similar in fact, that for our purposes we will combine them into a single persona — “neuro physicians.”
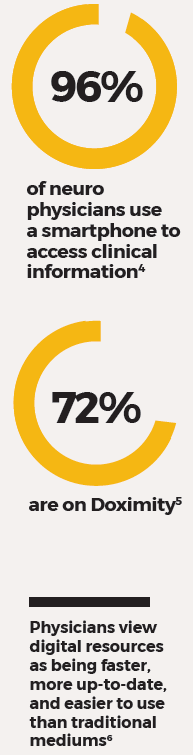
Technographics provide insights based on a person’s technology choices and use. By this measure, the data runs counter to the cliché that physicians are technophobes. The actual behavior of neuro physicians shows the reality (see column at right).
On mobile devices, there are a handful of medical apps neuro physicians use, each differently and at different frequencies. In line with their research habits, some apps, such as Epocrates and UpToDate, are being used on a daily basis. Meanwhile, others like Doximity and MedScape are used weekly for more in-depth research.
Neuro physicians are on social media. Facebook appears to be a guilty pleasure of sorts — it is the most used but least valued network. YouTube, on the other hand, is the most valued with these physicians. They watch videos to gain information about a specific procedure or treatment, for scoping out demos of new technologies, or to catch up on an event that they might have missed.
Speaking of events, physical conferences — of which neuro physicians attend two per year on average — remain important forums for dissemination and advancement of research, training, education, and networking. They are the number two source (behind the internet) physicians use to stay current in their specialty. But back to technology …
Whether on a computer or a smartphone, medical resources such as UpToDate and PubMed are consumed on-the-go for immediate answers and updates. Sites such as MedScape and AAN are being consumed less frequently, but are used for more in-depth findings and research.
Does medical literature still matter in this brave new world? Yes. To recap Doximity findings, 75 percent of physicians change their clinical practices quarterly or monthly based on reading medical literature. In this specialty, Neurology, Neurology Today and Neurology Reviews are most favored; however, there are others that are also widely read. But don’t necessarily think paper here — three specialties were found to be most likely to access clinical news through their phone or tablet: cardiology, orthopedic surgery and, yes, neurosurgery.
Psychographic dimensions
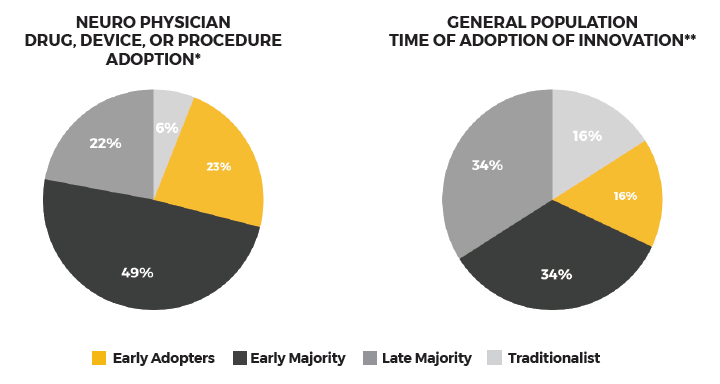
Neuro physicians are game to try new things (e.g., drugs, devices, or procedures7), especially compared with the general population8. However, motivation in these instances can be impacted by the innovation’s meaning. Clearly, a new treatment can have dramatic implications for people with brain disorders so neuro physicians may be highly motivated to try it to help their patients regardless of their personal risk-taking proclivities.
In any case, this type of analysis starts to cross over to behavioral and psychological layers that add further dimension to our personas.
Persona grata
So what does all this persona data mean? What does it matter if we know all we’ve presented here and more, down to what kind of car make neuro physicians prefer to drive most (Toyota at 18.5 percent)?
On a practical level, geographic, demographic, and technographic data can help improve media targeting and selection. This alone improves marketing efficiency and thus makes the persona construction effort worthwhile. But more than that, with psychographics, you can play “armchair psychologist” to improve your messaging.
For example, we know that neuro physicians view themselves as the elite of the elite. Yet, the autonomous, entrepreneurial role they have played in the past is changing. In much of the last decade, doctors in general have gone from being the lynchpin in the healthcare system to more of a cog in a larger wheel. That can lead to frustration, and the higher opinion of your abilities (neuro), the more the frustration. A forward thinking hospital can tap into this zeitgeist when crafting its appeals to this specialty.
You can play “armchair psychologist” to improve your messaging.
Carl Jung theorized that there are four primary psychological functions through which we experience the world: sensation, intuition, feeling, and thinking. His wife, Katharine Cook Briggs, and daughter, Isabel Briggs Myers, expanded this theory to create personality questions that would eventually turn into the Myers-Briggs Type Indicator (MBTI). This test produces a combination of four dichotomies:
- Extraversion vs. Introversion
- Sensing vs. Intuition
- Thinking vs. Feeling
- Judging vs. Perception
Most people are familiar with this test and know that it produces a four-letter personality type. For example, if you are ESTJ, that means you are primarily a sensing, thinking, judging extrovert. There are 16 different personality types in all.
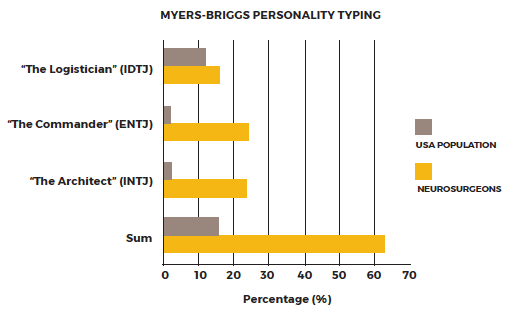
Various studies have been done linking medical specialties and Myers-Briggs personality typing. In the one below9 you can see that neurosurgeons can be categorized into three personality types (with the majority of those falling into two of the three). By looking at the sum of these three types, you can see how rare they are when measured against general population (last bars on chart).
Your top physicians — a double-edged sword
A point of consideration when building your institution’s reputation is your own physicians. In one study, specialists around the country rate only “outcomes” higher than “peers” when it comes to differentiators among top hospitals. In some ways, that makes reputation portable. If your specialty is tied heavily to a certain physician(s), that physician’s reputation goes to the next hospital when they leave. More focus on the multidisciplinary aspects of each specialty can help mitigate this. The reality is, though, it’s an “occupational hazard” for all providers.
Viva la difference?
According to another type of personality test, the Edwards Personal Preference Schedule, surgeons express “a need to be the center of attention in a group” more than their non-surgeon physician counterparts. We can only assume this would apply to neurosurgeons as well.
Getting personal
Adding personal narrative elements can help us complete our composite sketch of the neuro physician. In general, they are:
Extremely dedicated.
Their profession is a passion, a calling.
34% more likely to speak at a local professional event
37% more likely to teach at a medical school
25% more likely to review articles for peer-reviewed publication
32% more likely to author a blog or article for publication10
Statistics are in comparison to doctors in other specialties.
All consumed in their work.
They are so busy, in fact, that burnout in the field is a national concern (as is the nationwide shortage in this specialty).
2 out of 3 neurologists indicated their work schedule did not leave enough time for personal/family life
It is grueling beyond belief. Prepare for virtually no outside life. The 80-hour limit is a joke.”11
Insatiably inquisitive.
My oxygen is my colleagues and my intellectual curiosity,” said one.12 In fact, neurosurgeons read 30 publications on average. Neurologists, 29.13
Confident, some would argue, to a fault.
They talked about themselves and where they and their field stood in the world of medicine. They were, they said, still the jewels of hospitals and needed to demonstrate the worth of their procedures, to figure out a way, as one of them put it, ‘to have [hospitals] value [them] more than just for [their] good looks.’14
You have to have to deal with some bad problems. Most of them, hopefully, are not of your own making. But at some point, some of them are of your own making and then, what are you going to do? Are you going to quit? Are you going to crawl into a fetal position? In the end, everyone can have complications, and you have to learn from them, become a better surgeon, and move on.”*
Humbled by their profession.
They never forget a small mistake (or sometimes even no mistake) can end up with tragic consequences for the patient.
Implications for reputation building
The last step is to make your persona insights actionable by looking for the strategic and tactical implications that hide in the data. For example, in our consideration of neuro physicians:
They have sharp, fact-based minds, and a non-stop hunger for knowledge
Neuro physicians are always learning and constantly researching. This suggests using a blend of both “in-the-now media” and deeper thought leadership pieces that can be consumed in their discretionary time (what little of it there is). In either case, wrap your message to this group in a educational context to better the chance of it being seen. But remember to stay away from anything overtly promotional — they will see right through it.
They prefer autonomy and self-sufficiency to reliance on someone or something
Neuro physicians will gravitate toward/hold in esteem an institution that mirrors their bold, independent outlook. For example, do you have a “neuro vision for the future” (e.g., creating more pathways from the lab to the clinic to allow for faster progress? Advancing research lab capabilities to give physicians experience with innovations before they make it to the bedside?). Don’t be afraid to showcase new ideas or approaches to this specialty — they will likely be open to them.
Combine technology and traditional means to reach them
Neurophysicians are tech savvy, which makes them reachable on channels such as Doximity and Medscape, but they also like their in-person conferences. Geofencing, the use of GPS technology to create a virtual geographic boundary that enables a triggered response when a mobile device enters or leaves a particular area, can be used to target neurophysicians at physical events.
In summary
Don’t feel constrained to follow persona best practices (either the ones you’ve read about here or anywhere else). Your hospital or health system may have its own research, expertise, or experiential learnings that can and should be leveraged in this endeavor. Previous brand exposure/equity needs to be factored into the equation as well. Obviously, certain providers (e.g., ones located in Rochester or Cleveland) may have less work to do in the reputation-building area. For others, though, it may be time to start communicating directly to physicians nationally. But don’t wait too long — as a wise man once said, “Nobody ever built a reputation on what they were going to do.”
1 Santino Cua, Susan Moffatt-Bruce, Susan White. “Reputation and the Best Hospital Rankings: What Does It Really Mean?”, 1 Feb. 2017.
2, 3 Survey by reputation.com
4 Kantar Media. “Sources & Interaction: 2017 Medical/Surgical Edition Dashboard.”
5 Doximity
6 “Physician Perceptions Of Information Sources And Annual Reports Exploratory Research.” Movéo proprietary research, 2016.
7, 8 Sources & Interactions: 2017 Medical/Surgical Edition Dashboard Copyright© 2017 KANTAR MEDIA.
9 Everett M. Rogers. “Diffusion of Innovation.”
9, 10 Kantar Media. “Sources & Interaction: 2017 Medical/Surgical Edition Dashboard.”
11 SDN neurosurgery discussion forum answer to question, “How long and hard are the long and hard hours of neurosurgery?”
12 Janis M. Miyasaki, Carol Rheaume, Lisa Gulya, Aviva Ellenstein, Heidi B. Schwarz, Thomas R. Vidic, Tait D. Shanafelt, Terrence L. Cascino, Chris M. Keran, Neil A. Busis.”Qualitative study of burnout, career satisfaction, and well-being among US neurologists in 2016.” Neurology, Oct 2017. http://n.neurology.org/content/89/16/1730
13 Doximity
14 Charlene K. Petitjean. “Life, Love and Neurosurgery.” Project Wordsworth, 4 May 2013. Accessed from http://projectwordsworth.com/life-love-neurosurgery/
Author
Brian Davies
Managing Partner
bdavies@moveo.com
About Movéo
Movéo is a demand generation agency that focuses on three drivers of growth to help healthcare and B2B clients attract, secure, and retain more customers. For more information visit moveo.com.